Case of the Week #598
Associate Professor Obstetric and Gynecology, Zagazig University, Egypt.
A 25-year-old G1P0 woman with unremarkable past medical and family history was sent to our clinic at 15 weeks, 2 days gestation for the routine second trimester scan. The ultrasound scanning revealed the following findings.


View the Answer Hide the Answer
Answer
We present a case of diprosopus conjoined twin with craniorachischisis. The pregnancy was terminated.
Our ultrasound revealed the following findings:
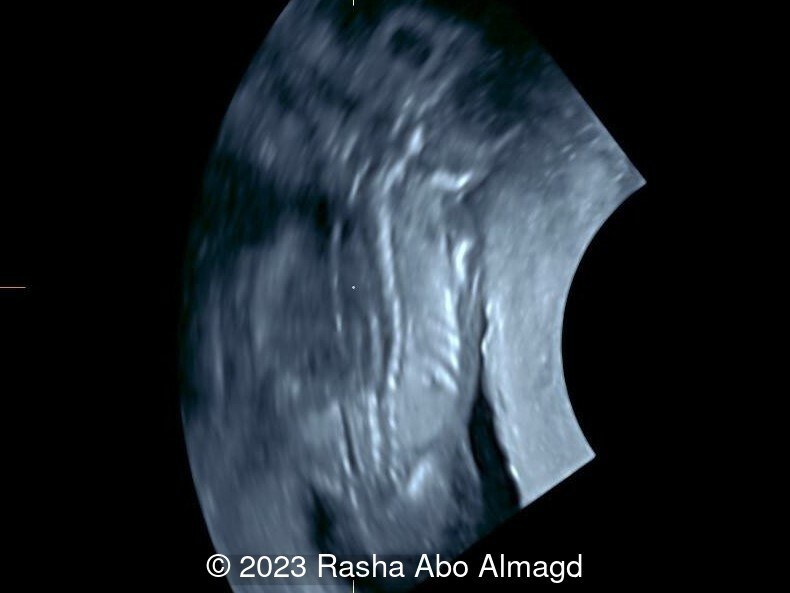
- Image 1: posterior coronal view of the fetal head demonstrating duplication of the cranium, absent skull vault (acrania), exencephaly of cerebral tissue, and rachischisis of the cervical spine.
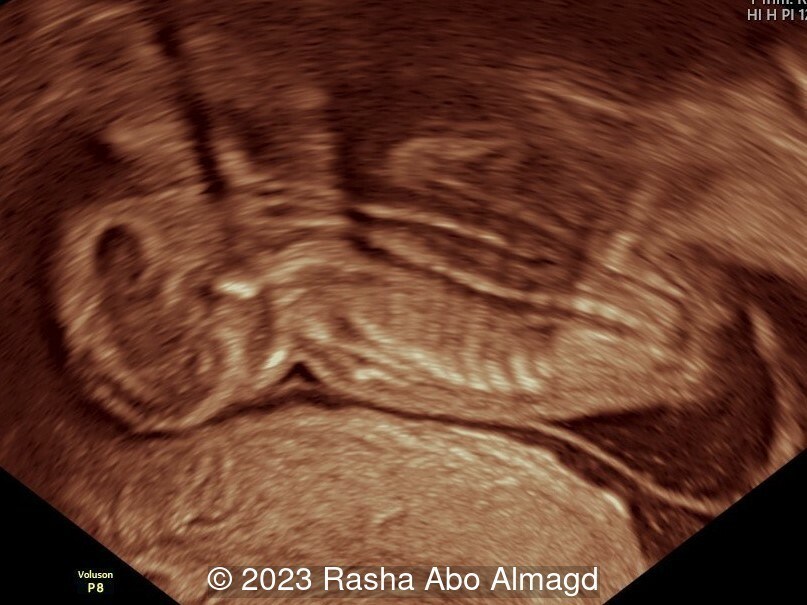
- Image 2: anterior coronal view of the fetal head showing a double face and frog eye sign.
- Video 1: Parasagittal sweep demonstrating conjoined twin Diprosopus (single head and double face), one trunk, dibrachius (two upper limbs), and dipus (two lower limbs)
- Image 3,4: complete rachischisis of the spine




Disscusion
Conjoined twins are a rare entity with an incidence of 1.47 in 100,000 births [1]. The diagnosis should be suspected when monozygotic fetuses are shown to consistently hold the same fixed position relative to each other. Conjoined twins are classified based upon the location of attachment [2]. The most common types of conjoined twins are thoracopagus (42%), parapagus dicephalus (12%), cephalopagus (6%) and omphalopagus (6%) [1]. The location and extent of fusion between the twins determines the potential for surgical separation and postnatal survival [2].
Diprosopus is a Greek term meaning duplication of the face. The patient typically has a craniofacial duplication with normal trunk and limbs, it is rare form of conjoined twins with reported incidence of 1 in 180,000 to 15,000,000 births [3]. In a classification described by Gorlin et al, all subjects have two complete oral cavities, but only 50% have complete facial duplication consisting of the presence of two mouths, two noses, and four eyes [4]. Cranial abnormalities, including anencephaly, craniorachischisis, brain duplication, agenesis of the corpus callosum, and encephalocele are very frequent in this type of conjoined twins [5]. In our case, complete duplication of the face and anencephaly was observed.
Conjoined twins are at risk for associated structural malformations, which impacts prognosis. Although shared organs can be visualized on gray-scale sonography, color flow mapping with Doppler can delineate vascular communications between the circulations. If significant, these vascular connections can lead to cardiovascular compromise and twin death. 3D ultrasound technologies can improve the accuracy of the diagnosis of conjoined twins and enable early diagnosis [6].
The prognosis of craniofacial duplication (Diprosopus) is unfavorable. It is essential to perform routine prenatal investigations to recognize these conditions early and differentiate them from other conditions affecting the midface and facial bones. Diprosopus should be considered in differential diagnosis of other conditions that affect facial bones and midface abnormalities such as supernumerary nostrils, medial cleft face syndrome, amniotic band syndrome, and lateral facial cleft [5].
Intrauterine fetal demise complicates over 10% of affected pregnancies and fewer than half of liveborn conjoined twins survive [7]. Early diagnosis of conjoined twins is important, as many patients will opt for termination because of the grave prognosis [7]. Beyond the first trimester, termination of conjoined twins can be technically difficult and in the third trimester, cesarean delivery is often necessary for patient safety.
References
[1] Mutchinick OM, Luna-Munoz L, Amar E, et al. Conjoined twins: a worldwide collaborative epidemiological study of the International Clearinghouse for Birth Defects Surveillance and Research. Am J Med Genet 157:274–287, 2011.
[2] Spenser R. Theoretical and analytical embryology of conjoined twin: part 2, adjustment to union. Clin Anat. 2000;13(2):97-120.
[3] D'Armiento M, Falleti J, Marutti GM, et al. Diproposus conjoined twins: Radiologic, autopic, and histologic study of the case. Fetal Pediatr Pathol. 2010;29(6):431-8.
[4] Gorlin R.J., Cohen M.M.J., Levin L.S. Syndrome of the Head and Neck. 3rd ed. Oxford University Press; New York, NY, USA: 1990.
[5] Trevisani V, Balestri E, Napoli M, et al. Diprosopus: A Rare Case of Craniofacial Duplication and a Systematic Review of the Literature. Genes (Basel). 2023 Aug 31;14(9):1745.
[6] Yang PY, Wu CH, Yeh GP, et al. Prenatal diagnosis of parapagus diprosopus dibrachius dipus twins with spina bifida in the first trimester using two- and three-dimensional ultrasound. Taiwan J Obstet Gynecol. 2015 Dec;54(6):780-3.
[7] Chen CP, Hsu CY, Su JW, et al: Conjoined twins detected in the first trimester: a review. Taiwan J Obstet Gynecol. 2011 Dec;50(4):424-31.
Discussion Board
Winners

Dianna Heidinger United States Sonographer

Javier Cortejoso Spain Physician

Pawel Swietlicki Poland Physician
Igor Yarchuk United States Sonographer
Andrii Averianov Ukraine Physician

Ana Ferrero Spain Physician

Alexandr Krasnov Ukraine Physician

Mayank Chowdhury India Physician

Ahmed Ezz United States Physician

Vladimir Lemaire United States Physician
Boujemaa Oueslati Tunisia Physician

Tatiana Koipish Belarus Physician
Bahauddin Sallout Saudi Arabia Physician
Marianovella Narcisi Italy Physician
Annette Reuss Germany Physician
Amparo Gimeno Spain Physician

Muradiye Yıldırım Turkey Physician
ALBANA CEREKJA Italy Physician
Eti Zetounie Israel Sonographer

Murat Cagan Turkey Physician

Sonio Sonio France AI
gholamreza azizi Iran, Islamic Republic of Physician

Hien Nguyen Van Viet Nam Physician
Subapriya Kandasamy India Physician
Mariam Bamanie Saudi Arabia Physician
Anette Beverdam Netherlands Sonographer
CHERYL TURNER United States Sonographer

Mai Phương Viet Nam Physician

Lynn Davis United States Sonographer

Ismail Guzelmansur Turkey Physician
zozo sichala Zambia radiology technologist

Amy Scheible United States Sonographer

Petra Barboríková Slovakia Physician

Le Tien Dung Viet Nam Physician

Tetiana Ishchenko Ukraine Physician
Costin Radu Lucian Romania Physician

Christina Pearson United States Sonographer
Molly Brown United States Sonographer

Gaurav Sharma India Physician