Case of the Week #644
UT Southwestern Medical Center, Plano, Texas, United States of America
A 34-year-old woman, G2P1001, presented to our maternal fetal medicine unit at 30 weeks of gestation for a late fetal anatomic survey. The fetus was female with low-risk noninvasive prenatal testing. The following findings were observed.







View the Answer Hide the Answer
Answer
We present a case of Vein of Galen Aneurysmal Malformation (VGAM).
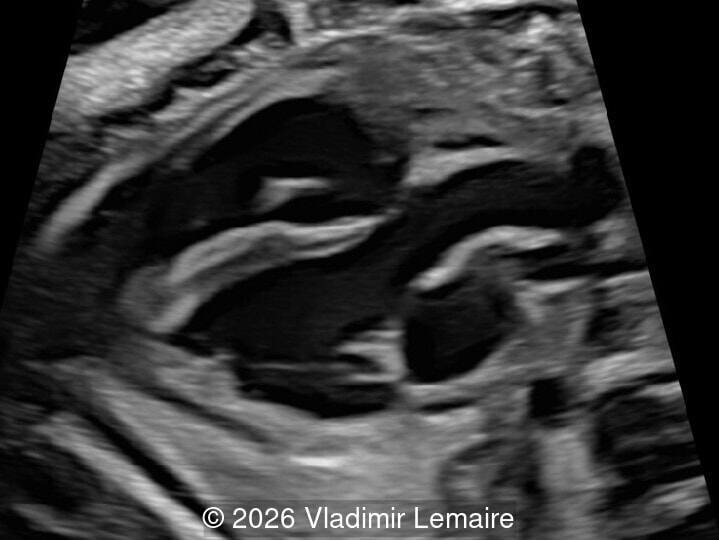
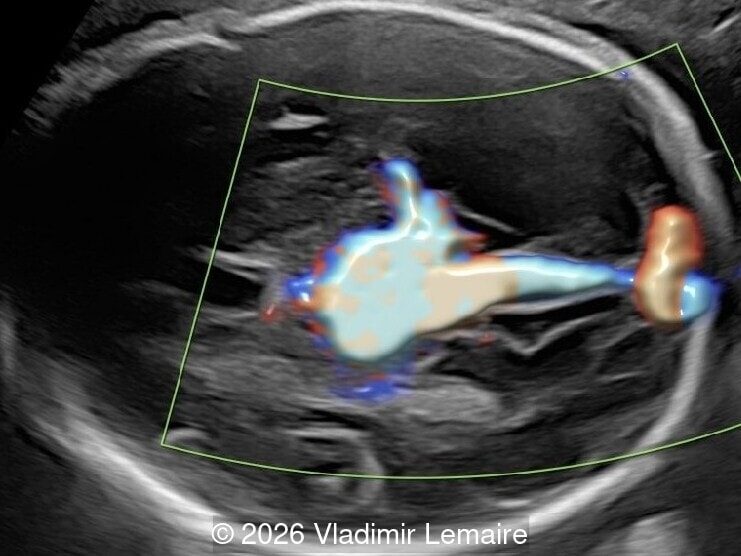
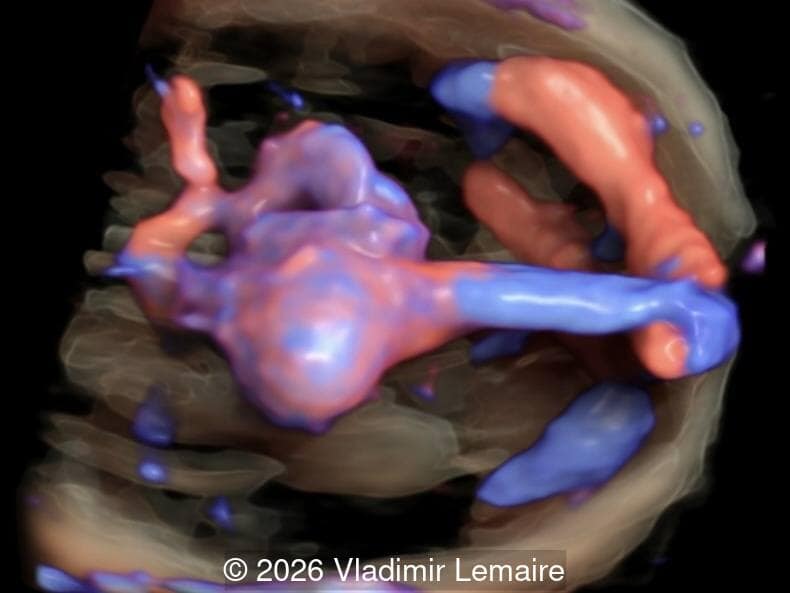
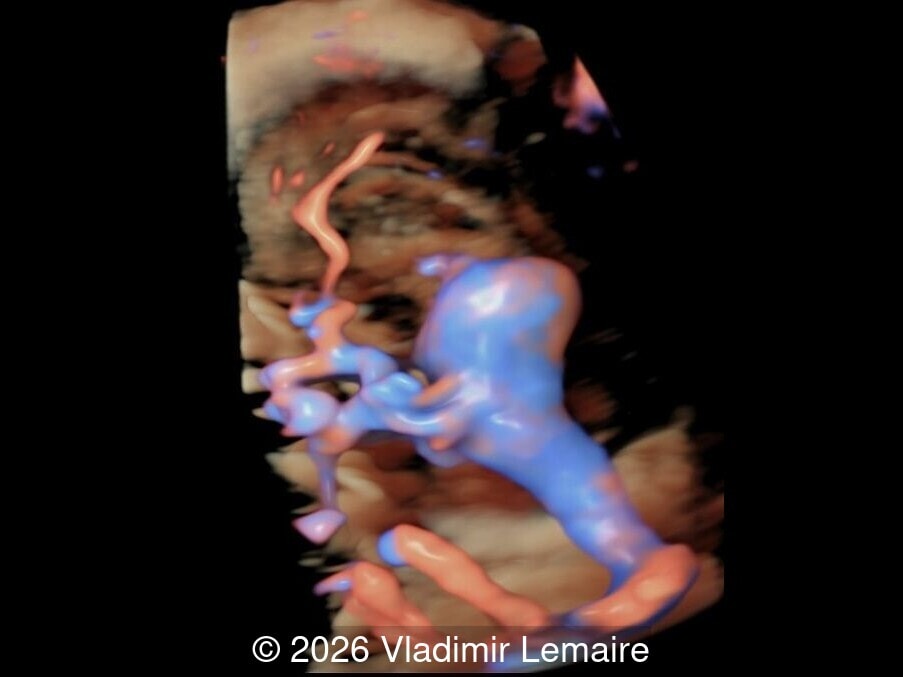
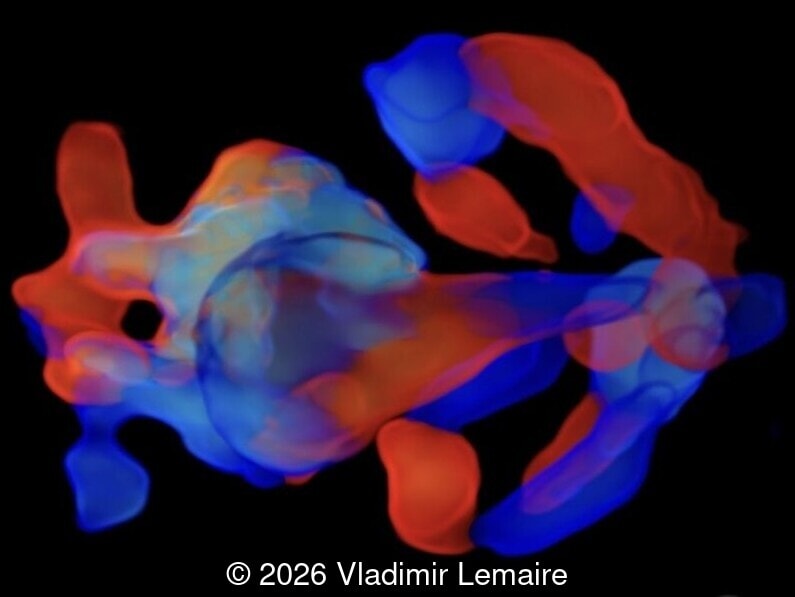
Our imaging revealed enlargement of the fetal heart with dilation of the superior vena cava. On further evaluation, we identified an elongated anechoic cystic structure in the midline of the head, without mass effect on the surrounding structures. Color doppler demonstrated an arteriovenous fistula between the deep choroidal arteries and the embryonic median prosencephalic vein of Markowski. The vein of Galen aneurysmal malformation was likely the contributing factor to the cardiac enlargement. Cardiac function was, however, preserved and hydrops not present. Additional images are shown below.


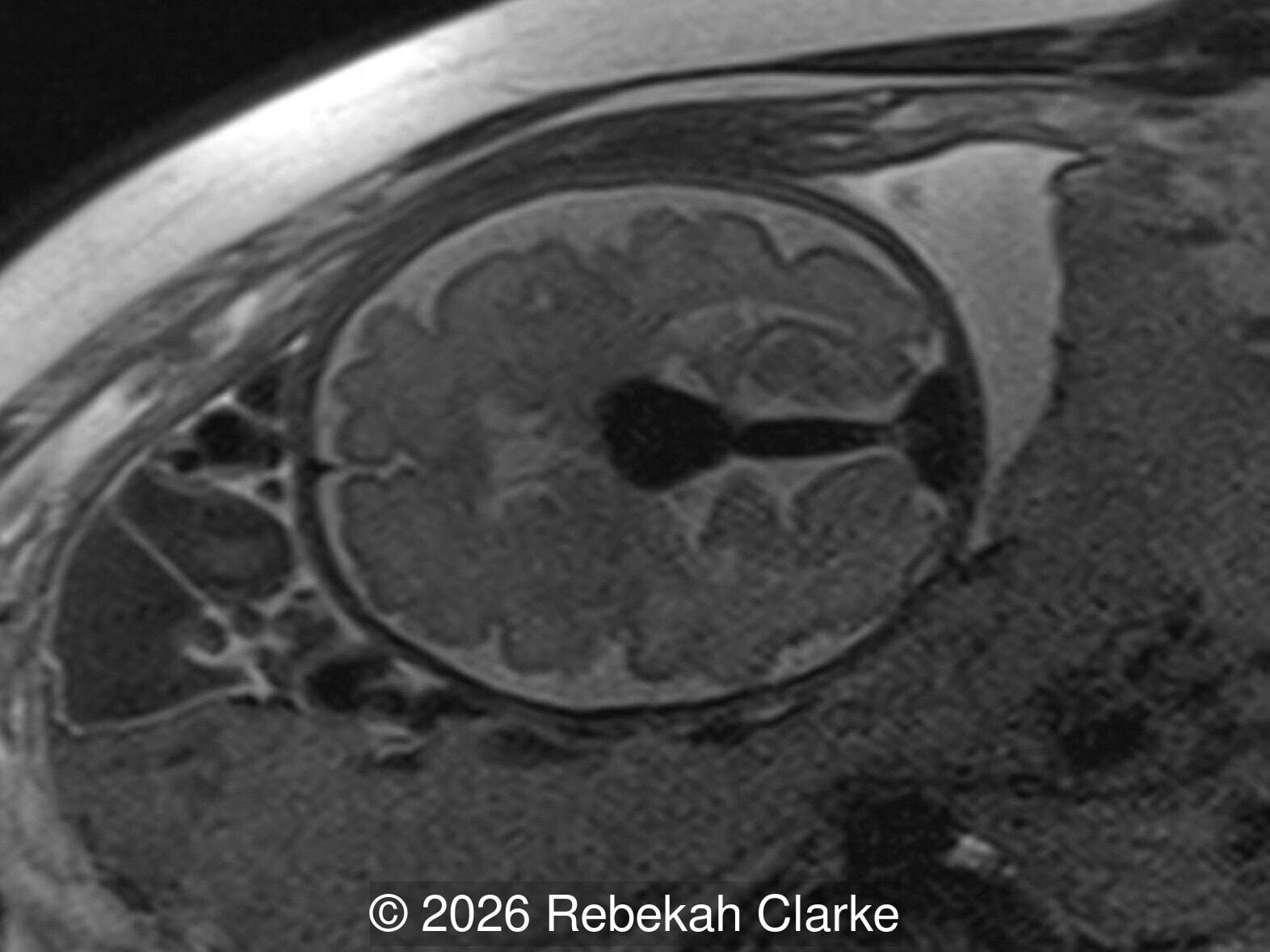
The diagnosis was confirmed by fetal magnetic resonance imaging (MRI). Our patient did not meet the criteria for in utero embolization. At 37 weeks she was delivered via cesarean section and underwent postnatal embolization.

Discussion
A vein of Galen aneurysmal malformation (VGAM) is a space-occupying lesion that results from an arteriovenous fistula between deep choroidal arteries and the median prosencephalic vein of Markowski. The vein of Markowski drains into the vein of Galen, thus the lesion is not a true aneurysm, but the term is still commonly used to describe this fistula. A VGAM is rare and accounts for less than 1% of all vascular malformations. It is, however, the most common type of arteriovenous malformation in the fetus. A VGAM is present in the first trimester, between weeks 6 to 11, but its effects such as dilation, cerebral compression, and cardiac volume overload may not be seen until the second and third trimester.
On ultrasound, a VGAM appears as an elongated anechoic cystic structure in the middle of the head, often without mass effect on the surrounding structures. Color Doppler shows high-velocity flow in the lesion and can be used to identify the arteries feeding the vascular malformation. Pulsed-wave Doppler shows markedly turbulent flow. Additional key echocardiographic features include an enlarged heart with preserved systolic function, a dilated superior vena cava, and mild or moderate tricuspid regurgitation. Tricuspid regurgitation was not present in our case at the time of our evaluation.
The normal combined cardiac output in the fetus is approximately 400 to 500 ml/Kg/min of flow. The fetal cardiovascular system can tolerate volume loads as high as 700 to 800 ml/Kg/min of flow. In a VGAM, up to 80% of the fetal cardiac output may be redirected to cerebral circulation leading to high-output cardiac failure and hydrops. Due to mass effect, a VGAM may also be associated with secondary hydrocephalus, brain hypoplasia and altered cerebral development. Cerebral hemorrhage and thrombosis have also been reported.
In utero embolization of high-risk VGAM with a falcine sinus width of 7 mm or greater is now feasible as reported by Orbach et al. In a single-group intervention study, 5 of 7 patients underwent successful embolization. Three of five embolized patients survived past the neonatal period, all without neurodevelopmental delay. Postembolization magnetic resonance imaging (MRI) showed no clinically significant parenchymal injury.
Differential diagnosis includes dural sinus arteriovenous malformation, venous sinus engorgement, arachnoid cyst, and porencephaly.
References
- Chaoui R, et al. "The Intracerebral Vascular System in 3D Glass-Body Mode". 3D Ultrasound in Prenatal Diagnosis: A Practical Approach (2nd edition). Berlin, Germany: DeGruyter, 2024. pgs 251-253.
- Doubilet P, et al. “Vein of Galen Aneurysm”. Atlas of Ultrasound in Obstetrics and Gynecology (third edition). Philadelphia: Wolters Kluwer, 2019. pgs 87-89.
- Orbach DB, Shamshirsaz AA, Wilkins-Haug L, et al. In Utero Embolization for Fetal Vein of Galen Malformation. JAMA. 2025 Sep 9;334(10):878-885.
- Paladini D, et al. “Central and Peripheral Nervous System Anomalies”. Ultrasound of Congenital Fetal Anomalies: Differential Diagnosis and Prognostic Indicators (second edition). Boca Raton: CRC Press, 2014. p 79.
- Rychick J, et al. “Cerebral Arteriovenous Malformation”. Fetal Cardiovascular Imaging. Philadelphia: Elsevier, 2012. pgs 443-450.
- Woodward P, et al. “Vein of Galen Aneurysmal Malformation”. Diagnostic Imaging Obstetrics (fourth edition). Philadelphia: Elsevier, 2021. pgs 190-193.
Discussion Board
We appreciate your patience as we review all submitted answers. Check back soon to see if you were correct!